“This amounts to creating a new way of stigmatizing those who lack in self-sufficiency and in positive thinking. Not only is lack of self-worth not viewed as an effect of social structure but it is viewed as self-inflicted”1
–Dr. Eva Illouz, on the stigmatization caused by positive psychology

Stigmatization against people who are mentally ill is rampant in our society, no matter how many articles from popular magazines we get in our news feeds touting the contrary. There is a deep history of such negative stereotyping spanning millennia. Today in the United States it’s at least generally understood how harmful those stereotypes are, and efforts in the medical world and in psychology are being made to help overcome those barriers in care settings.
The primary cause of stigma is unfounded fear—a fear that is all too often shaped by the media nowadays. (See also the post on stigmatization and the media.) Stereotypes can be overcome, however: studies show that exposure to patients with mental illness, or even just providing accurate information about mental illness, can alter perceptions of a demographic like nursing students, all of whom in one study answered “the media” when asked where they had formed their original negative opinions about people with mental illness (PMI).
People with a mental illness have been stigmatized since the beginning of recorded time. Even the word stigmatization is steeped in historical tenebrosity: In ancient Greco-Roman times a stigma was a tattoo (also an iron brand in Rome) used for slaves and criminals, derived from the Greek stem “stig,” which means to prick. 2 There was no love for those of lower status in antiquity: “Slaves are… regularly and scornfully referred to with words such as literati (lettered), stigmatici (tattooed), inscripti (inscribed), and graptoi (written upon).”3
Sufferers from mental illnesses at the time of Cicero (106-43 BC) would find themselves placed into one of two categories, just as they would today: is it a serious mental illness (SMI) or a less-threatening mental illness? The belief at that time was that having a “mild” mental illness was a moral failing, whereas serious mental illness meant the sufferer was besieged by angry gods or demons.4
Interestingly, I have been given a first person account that there are contemporary evangelical churches which espouse one if not both of these beliefs. I took a class with an employee in the air force, and she explained how her church treated her panic disorder as if it were her fault. She wasn’t in prayer enough, apparently.
It’s worth noting that Asclepiades (129/124 BC – 40 BC) turned his back on Hippocrates’s humours—the prevailing medical view at the time. “Asclepiades advocated for fresh air, light, appropriate diet, hydrotherapy, music therapy, massage, and exercise rather than darkness and torture for individuals with mental illness.”5
At that time, treatment for PMI included cold baths and emetics; (vomitus or other bodily fluid appearing was a sign that the herbs and drugs were working). It did, however, also include torture and in some cases being put to death. My guess is those with thought disorders like schizophrenia probably fared worse during those times than those with cyclothymia. But what a revolution Asclepiades brought about!
Greek physician Aelius Galenus, (aka Claudius Galenus: 129–216 AD) set the scene for the Medieval Ages. Galen’s thoughts on medicine dominated and influenced Western medicine for over 1,300 years. Hippocrates’ ways maintained their mainstream status, meanwhile, an asclepion became a sanatorium for the sick to be ministered by the priests. Through vivisection Galen learned a great deal about anatomy. Further, “he learned the importance of diet, fitness, hygiene and preventive measures, as well as living anatomy, and the treatment of fractures and severe trauma.”6
Much of the academic research is limited to the texts found, which reveal “mental illnesses” as melancholia, love-sickness, hypochondria, grief, and even lycanthropy.7 Possession by demons was most certainly a diagnosis during these times. And persecution by the Church only grow fiercer.
During the Middle Age, it was falsely believed that a SMI was a deliberate affliction from God—that He had marked those in consort with the devil with such an ailment. Those men and women were destined for madhouses, which had been erected to hide the shameful mentally ill away from society until their death. Another option was being burned at the stake if the illness included any delusions or manifestations that were particularly troubling and therefore an indication one was indeed possessed by a demon.
The notion that the Middle Age was particularly tough for the mentally ill, who faced religious persecution, is not universally adopted. Kroll and Bachrach8 examined 57 depictions of mental illness from saints and pre-Crusade chronicles. They determined that only 16% of the descriptions sourced the mental illness as being sin against God.
According to the Middle Age sources they consulted, mental illness was generally understood as being caused by humors à la Hippocrates, as well as bad diet, too much alcohol, overworking, and grief. It was considered a truism that God creates all things, therefore he creates mental illness also. Contrary to this humane position (from an extremely small sample size) are accounts like these:
Medieval Europe, along with its medicinal practices was overtaken by Christianity. That meant more exorcisms, more chants, more torturing. During the Early Medieval Ages people still believed that the fluids [the humours mentioned above] were the ones that caused mental illness, and in order to bring balance back to the body, patients were given laxatives, emetics, and were bled using cupping or leeches.9
That doesn’t sound especially bad, unless you realize that while one PMI was headed for a laxative and a few leeches, another was being burned at the stake.
Another process asserted its place in history during this time.—trephining. Trephining is a process in which a doctor cracks a hole in the ill person’s skull to “let the evil spirits come out,” (as first conceived). It’s depicted as a peaceful process in the following picture:

In some parts of the world “doctors” (priests) would try exorcism, or threaten the spirit, even “forcing it into submission.” Of course the patient was the receptacle for all this abuse. Unfortunately, we have multiple types of mental illness, and we can’t know how priest-doctors treated each one.
What we do know is that in the Enlightenment period, the stigma started to budge just a little. Trephining was no longer to let the evil spirits out, but was a precursor to modern brain surgery. Physicians didn’t know what they were cutting out, so many patients ended up with terrible results, from drooling to catatonia.
Despite small gains, the stigmatization was very much out in the open: Bedlam, which is a psychiatric facility in Britain today, was notorious during this time for housing “the insane.” The first state-sponsored American asylum was Worcester State Hospital in Massachusetts in 1833. By 1860, 28 out of the 33 states had mental hospitals.
Unfortunately, World War II engendered a new peak in stigmatization: Nazis murdered and sterilized hundreds of thousands of sufferers.11 Psychiatrists played a large role in the orchestration of the extermination: “It was psychiatrists who reported their patients to the authorities and coordinated their transfer from all over Germany to gas chambers situated on the premises of the six psychiatric institutions: Brandenburg, Grafeneck, Hartheim, Sonnenstein, Bernburg, and Hadamard.” 12 Worse than orchestration, however:
It was psychiatrists who coordinated the “channeling” of patients on arrival into specially modified rooms where gassing took place. It was psychiatrists who saw to the killing of the patients (initially using carbon monoxide and later, starvation and injection). Finally, it was psychiatrists who faked causes of death on certificates sent to these patients’ next of kin. It has been estimated that over 200,000 individuals with mental disorders of all subtypes were put to death in this manner.13
The atrocities afflicted against the mentally ill largely took place before Jewish persecution. People with a mental illness were useful lab rats for Hitler’s “final solution,” however. And even though around 200,000 mentally ill people perished at the hands of the Nazis, we can never forget Hitler’s party exterminated 6 million Jews. During this time in America, conscientious objectors entered the state mental hospitals to cover for the doctors sent away for the war effort.14
The 1940s saw significant stigma. In 1946, Life Magazine published photos that depicted the horrors of mental institutions.
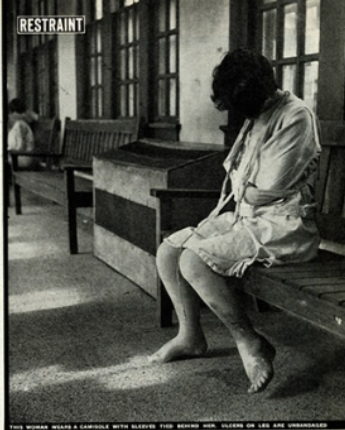
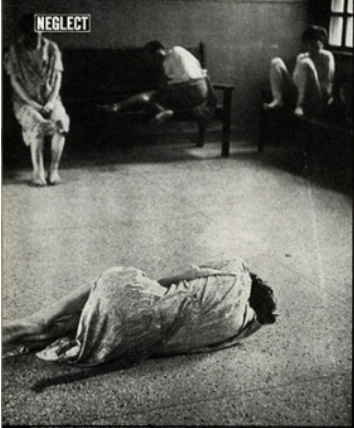
Images from KQED.org15
In the 1950s the high level of stigma largely remained. Mental illness was not thought to be curable or effectively treatable, so society still locked up the “lunatics” in asylums.16 In 1955 the number of PMI who were institutionalized reached a peak of 560,000; a few years later in 1959 the number of PMI institutionalized in California peaked at 37,000.
Attitudes began to shift in the 1960s. In 1963, President John F. Kennedy signed the Community Mental Health Act—officially known as the Mental Retardation Facilities and Community Mental Health Centers Construction Act, which started to push the responsibility of PMI from the state toward the federal government. JFK wanted to build a network of community mental health centers so that PMI could live in the community while receiving care. He was possibly inspired by his mentally ill sister, who was lobotomized and spent the rest of her life hidden away from society.
Less than a month after signing the bill into law, JFK was assassinated, and his dream of psychiatric community centres never came to fruition. Even now, some states contain these community-style “half-way houses.” If you ever read We Heard the Angels of Madness, the narrator’s son, whose severe bipolar disorder came on while he was a college student, ends up finding a home in such a place. The book is a good one, as it’s honest—full of heartache—and informative, especially for those who know little about bipolar disorder. It’s very difficult to find a place in one of these living facilities, and some states don’t have any such resources.
I had a great aunt—the sister of my now 102-year-old grandmother who is still alive out of sheer irascibility. As a child, my great aunt used to show up inside other people’s homes: she’d just walk inside. She wasn’t there to steal anything or to frighten anyone. She was tragically ill. She was institutionalized for the rest of her life, and my grandmother wouldn’t speak of her—she never has.
In 1967, Ronald Reagan became governor of California. The number of patients in Californian state hospitals had dropped to 22,000, perhaps because of the shifted sentiment around mental illness. Reagan took the opportunity to make cuts in the Department of Mental Hygiene. Ten percent of the budget was slashed, and 2,600 people were let go despite reports indicating that hospitals were operating below recommended staffing levels.
The same year, Reagan signed into law the Lanterman-Petris-Short Act, which ended much of the involuntary institutionalization of patients. Unfortunately, many of the patients who left the hospitals following the bill’s passage were too ill to enter society. Homelessness soared. And the year after the law went into effect, the number of PMI who entered San Mateo’s criminal justice system doubled. Soon there was a full-blown crisis, and in 1969 Reagan reversed his earlier cuts.
The 1970s saw a continuation of public goodwill. A movement started that called for the rehabilitation of PMI rather than putting them away. In 1978, President Jimmy Carter set up a commission to investigate the status of PMI, and he then passed the Mental Health Systems Act (MHSA) of 1980. This legislation, which had been introduced the year before by senator Ted Kennedy, was heralded as an unprecedented victory for the mentally ill and their supporters.
Being a Kennedy seems to come with pain as well as privilege: “Patrick Kennedy, son of the late Senator Ted Kennedy and nephew of both Bobby Kennedy and JFK, said he believes witnessing his brothers’ murders caused his father to suffer from PTSD.”[17]
The following year, President Ronald Reagan repealed most of the MHSA via reconciliation. It was said that congress felt state provisions for PMI were adequate without federal involvement. The “patients’ bill of rights”—section 501 of the MHSA—was not repealed, but rather left in place to give states a reminder to tweak their own systems. It doesn’t take much imagination to determine what happened to people with an SMI who lived in a poor state without any federal aid after that.
My great aunt was committed in England, where I grew up. The iron-hearted Margaret Thatcher was elected in 1983, the same year that saw the landmark legislation the Mental Health Act. It set guidelines for who could be hospitalized against their wishes (called “sectioning”.) If someone is sectioned, they have the right to appeal and the right to receive help from an independent advocate.
It’s sad to say that not much ground has been gained against eliminating mental health stigma since the 1980s. In 2004, the US Department of Justice estimated that 10% of state prisoners have symptoms that meet criteria of a psychotic disorder. And the Los Angeles County jail is now known as being the largest mental health institution in the country. The jail population has more than doubled in the last ten years. One facility for men—the Twin Towers in downtown LA—is now dedicated almost entirely to inmates with mental health issues who are under moderate or high observation:
The men in high observation – numbering about 1,000 – reside in Tower 1. When they are not in their cells, they are handcuffed to metal tables so they can’t harm themselves or others, and many are dressed in quilted robes to prevent self-harm. They live in pods of 16 cells that are often noisy and foul-smelling.18
It doesn’t sound very humane, does it? I’m always surprised at how punitive this country is—I don’t know why — I’ve been living here long enough. But of course systemic racism plays a large role.
Today, more than five decades after the Lanterman-Petris-Short Act (LPS) became law, California still lacks a system of community mental health care, as several people testified on Wednesday, December 22, 2021. “We wouldn’t be here if this thing were running like a clock. Clearly, there are serious, serious challenges,” Assembly Health Committee Chairman Jim Wood, a Santa Rosa Democrat said as the hearing progressed. “We have a huge breakdown,” said Sen. Susan Eggman, a Stockton Democrat who has carried legislation to plug some of the gaps, and intends to push for more.
A letter from so many years ago to Assemblyman Frank Lanterman begged, “We wish to ask, therefore: Does a crime have to be committed before the one who is ill can be once confined for treatment?” Because therein lies the rub: although it is good that the bar to commit someone is high—involuntary commitment should be reserved for someone about to hurt themselves or others—parents were (and are) unable to get their unstable adult children the help they need. Family and other loved ones have to watch a PMI deteriorate to a dangerous level before they can be committed. From that letter: “Treatment is not a bad word.”19
I have been involuntarily committed twice. Both times I was so heavily drugged I hardly remember a thing. It was at a psychiatric facility called Charter, operated by Kaiser Permanente in California. It closed down—whether for financial reasons or those more consistent with my extremely unpleasant experiences with them, I do not know. I have no idea if my lived-in sense of the passage of time was accelerated, or the opposite. How fast does time go when you’re drooling in a corner?
The first time I was committed was in my early twenties, when my illness really started to take off in a frightening direction. I had just graduated with a Masters in Linguistics. I had recently become homeless through a series of life choices I still don’t regret, the main one falling in love with the man who would become my first husband.
It was Thanksgiving. The man—we’ll call him Tom—drove to my parents’ house in the East Bay after I was committed. He brought my mother flowers and broke the news to her of where I was. As much as her heart was breaking, at least she could make a fuss over this young lad she’d never met before. She gave him clothes from my foster brother who was at least a foot taller while she washed his clothes in the machine, and she gave him homemade Greek bean soup.
The days leading up to my commitment hadn’t been pleasant for us. On Thanksgiving Day, which, being British, I don’t celebrate, Tom brought my best friend and employer to have lunch with him and me at the hospital. I was anguished! I didn’t want anyone knowing about my “dirty little secret.” I didn’t want anyone to know I was hospitalized. I was full of misplaced shame and so angry with my boyfriend. The poor chap was trying to boost my spirits with our guest, and all I could think was that now my best friend knew I was seriously mentally ill.
I have also gone to the hospital voluntarily for emergency mental health services at a different facility. I check in at the front with an, “I’m bipolar and I want to end my life,” and the next thing I’m ensconced in the waiting room for hours while I wave at the guard with a gun who has slipped inside to discretely monitor me. The poor sod stands against the wall for hours and hours. Later I’ll be moved to a room, and the poor guard has to play Angry Birds on a chair outside for umpteen hours until on-call psych arrives. On those occasions, upon being admitted, I am given a copy of all my admission paperwork, as well as a printed patients’ bill of rights, as soon as I get to my room.
I have to authorize their use of each of my medications. I balked once at the amount of haloperidol they wanted to be able to give me if necessary, but eventually caved. Later I heard the nurse crow to her superior that she had convinced me to sign the form, like it was a feather in her cap. Stanford Hospital used to have incredible nurses, but cutbacks mean the best have left, and patient care is inferior to what it was. I had a nurse fifteen years ago predict the shortage of nursing and drop in care that would be to follow, and she was dead on. Some of my hospitalizations were short, and some longer. I’m sure I’ll write more about those in the future.
I was deep in hiding. (Am I not now?) I’m afraid what will happen if the whole world knows my diagnosis. I have typically been high functional, so my sickness isn’t on full display like it is for my friend Yoko. She is schizophrenic and a piano prodigy. We bonded over similar levels of dysfunction and rare stomach diseases. I have chronic idiopathic intestinal pseudo-obstruction (CIIPO), which means I don’t “go” unless I have a lot of laxative medicine. She had gastroparesis, causing her to throw up everything, including water. Whereas I was believed and treated (eventually), Yoko was spurned.
After my friend couldn’t keep anything, including water, down for several days, I got worried that she might get dangerously dehydrated. I convinced her to take the bus to the hospital. Later I checked my voicemail, and what I heard broke my heart: “I thought the stigma was supposed to be over,” Yoko wailed into my phone. The triage nurse had simply taken one look at her, literally rolled her eyes, and said on the phone to another nurse in a sarcastic tone, “patient is schizophrenic.” And she was not taken seriously after that. She was mortified and defeated.
The stigma is still very pervasive. Even with all the recent educational material published, PMI face enormous hurdles. For the first time research shows the stigma toward depression has eased. But it has actually increased for all other mental illnesses.20
A December 2021 study published in JAMA Network Open examined how stigma has changed over the past two decades for mental health disorders such as schizophrenia, major depressive disorder and alcohol use disorder. Indiana University researchers used data from the U.S. National Stigma Studies, which are part of the General Social Survey, to examine public stigma over a 22-year period at three key points: in 1996, 2006 and 2018.
The study found that from 1996 to 2006, Americans reported increasing beliefs that mental illness is caused by genetics or chemical/physical disruptions in the brain, rather than moral causes like having a faulty character or bad upbringing. While these findings reflected a greater belief in scientific causes, they were not accompanied by any decrease in the public rejection of those with mental health issues.
However, data from 2006 to 2018 showed a statistically significant drop in social rejection for people with depression. Across a number of social contexts, including the workplace, the family and the neighborhood, fewer Americans in the 2018 study compared to the 2006 study expressed an unwillingness to interact with the people described as having the mental illness.
Other disorders did not see any reduction in people’s desire to avoid the sufferers socially, however. In fact, public perceptions attributing dangerousness to schizophrenia and lack of morality to alcohol use disorder saw a troubling increase.
When it comes to stigma, the study found there were few differences across subgroups including gender, education and income. The authors documented the well-known “conservatizing effect of age,” i.e. the increased likelihood of holding more stigmatizing attitudes or “conservative values” as one gets older. They further noted indications that some birth cohorts, including the opposite-in-age “greatest generation” and millennials, hold less stigmatizing attitudes and beliefs. The researchers speculate that different experiences of these groups early in life may be at work.21
The researchers had multiple recommendations to address the importance of mental health, including leveraging the educational system to introduce level-appropriate information on mental health, as well as providing teachers with high-quality materials for mental health-related courses.
Of course, some schools have been trying exactly this approach and have met with rabid opposition from MAGA parents whose own education is obviously very lacking, given they think “exposing a child” to mental health information “introduces dangerous ideas like suicide and depression” to their kids. They believe they have to sole right to decide what their kids are taught. By the way, this is a uniquely American attitude, and not one this country should be proud of. Other countries raise children. A large swathe of Americans just wants to own them.
A significant perpetuator of the stigma currently is MAGA parents: “Groups have voiced opposition to suicide prevention programs, mental health coordinators, and social emotional learning, claiming that they are being used to indoctrinate students.”22 It’s hard for someone with any education to relate to this type of thinking at all.
Why would anyone believe that depression is “infectious,” and transmitted via honest discussion? It’s a bit distressing to know that parents of innocent children are perpetuating the stigma that sufferers, their relatives, and independent researchers all say is so very harmful.
One privileged yet quite incorrect parent at a board meeting said, “At Carroll ISD, you are actually advertising suicide…. Some of these kids, they’re just trying to get through the day, get through compacted math, get through algebra, go to cotillion on Sunday. They are not thinking about these issues.”23
Currently, approximately one in six school students have enough behavioural or emotional problems to be diagnosed with a mental disorder.24 The average public school enrollment is 527 students. Eighty-seven students aren’t “not thinking about these issues.” And 87 students deserve to be treated well, with compassion and understanding. The last thing they need are idiot parents with their own piggish agendas. They should just homeschool their children and leave the real schooling to those with no intentions of perpetuating harmful stigmas.
In a few years, or perhaps longer if we’re unlucky, we will hopefully see a remission of the MAGA parents and greater school involvement with their students on topics that affect PMI. Social emotional learning is designed to cultivate empathy in students. Hopefully those who are exposed to the topic of mental health early and often enough, with support from parents and teachers, will be the cohort that defeats stigma. It might stay ugly until then—there is no sign of the MAGA nastiness subsiding any time soon.
A second perpetuator of the stigma is “science”, and this is equally tricky to understand. There was a ripple of headlines recently that ran along the lines of “Schizophrenia linked to violent behavior, but experts push back.” Here’s what happens when you reduce a complicated spectrum of illnesses (schizophrenia spectrum disorder — SSD) that manifests differently in each person to a single data point for meta-analysis.
Firstly, do you know how the researchers got their data? Mostly from public registries, implying this specific population is already criminally-minded. That’s a feature of this sort of research—taking populations from prison databases or other criminal databases. It rather makes you think wonder about all the people with SSD who are not in these databases. Are they more likely to be violent? Perhaps there are some compounding factors to the schizophrenia. I’m guessing that for people in prison in the United States or the United Kingdom this is definitely the case, as the two punitive countries are more likely to damage someone’s self than rehabilitate it.
Furthermore, dual diagnosis was noted for the statistics released (mental illness — e.g. borderline personality disorder — Yet somehow the higher numbers got precedence for publication. I wonder what percentage of the “regular” population who are dual diagnosis and in public registries were violent?
That would have been called a control group in most scientific studies, but this meta-analysis of 24 studies involving 51,309 people with SSD from 15 countries over four decades didn’t care whether the studies had controls. In fact, a feature of these studies is they don’t care what comorbid details they drag into their study, as long as that “schizophrenia” checkbox is crossed.
The researchers appear to hold some particularly malignant views about people with schizophrenia spectrum disorder, however:
“I think one of the key implications of this study is that violence outcome prevention really should be a focus for clinical services because these are important outcomes to prevent and many of the factors that increase risk can be changed, such as substance abuse and treatment adherence.”
study co-investigator Seena Fazel, MD, professor of forensic psychiatry at the University of Oxford, United Kingdom
Violence outcome prevention…? These scientists have some pretty rich notions about those with SSD! Although the United Kingdom isn’t known for its tolerance of PMI. People with SSD are not simply dangerous people out to get drunk, homeless, and stop taking meds. Even if they were, it is their right to live their (nonviolent) lives as they wish.
We have no right to force medical treatment on someone else. Yes, it can be painful when someone goes off their meds and does seem to “go crazy.” Believe me, I know from both ends. But that’s the tragedy of it; we think we know what would make someone better, but we’re not that person. We’re not in their head. That’s not to say help shouldn’t be offered. And if that slippery slope hits the rocks, then there is sectioning, or involuntary commitment.
It’s not unusual for newspapers, regional and national, to write stories from science studies if they have salacious details. And what’s more titillating than a propensity of people with SSD to become violent? The newspapers and other publications often don’t interpret the science correctly, even when copying from the original publication. (That would be an article from Medscape which is behind a member-only wall. And to be clear, you have to be a health care professional (not a researcher) to get behind that wall.)
Still, the source (solozair) that I used seemed like a solid interpretation of the study results with some due diligence: “Previous exposure to violence, childhood trauma, or other known risk factors were not included in the study.” Well, they should have been. And the control groups should have had the same risk factors.
Fortunately, the article explains the important detail that correlation is not causation. That is, it’s simply not proven that people with SSD are more likely to be violent; rather, researchers noticed from criminal databases that people with SSD are associated with increased violence. The difference between coincidence and causality is a significant one, and these studies are often interpreted with causality when just a link has been established.
Unfortunately, the article from solozair continues on to list data without context. And let’s be clear again, there were many limitations to this study. Since it’s out there, here it is for your reading pleasure:
- The risk of violence committed by men with schizophrenia was 4.5 times higher (95% CI, 3.6-5.6) than their counterparts in the general population. In women, the rate was 10.2 times higher (95% CI, 7.1 – 14.6) than in women without SSD. The probability of committing sexual offenses (odds ratio [OR], 5.1; 95% CI, 3.8 – 6.8) and homicide (OR, 17.7; 95% CI, 13.9 – 22.6) were also increased.
- Absolute risks of assault ranged from 2.3% to 24.7% in men with SSD and from 0% up to 5.4% in women up to a 35 year follow-up.
The head researcher, Seena Fazel, has an opinion about these statistics: “That means that over a 35-year period, most men will not be involved in these criminal record-based violent outcomes,” Fazel said. “And at least 90% of women won’t have registry-based violent outcomes.” Such confidence in these numbers.
The researcher Daniel Whiting, BM BCh, a doctoral researcher in psychiatry at the University of Oxford, told Medscape Medical News:
An important way to consider the association is to think of clinical services for people with schizophrenia spectrum disorder: does the evidence suggest that violence is a significant enough potentially adverse outcome for a minority of those individuals that support for this clinical should be improved?”
How about we up the services for people with SSD regardless of whether you can show they are associated with higher rates of violence? We should improve the standard of care regardless. It really takes a threat of “violence” to show that adequate care should be provided with those with SSD?
Do you know what I really want to know? How many of those “violent” sufferers of SSD have been assaulted? Please include that among your checkboxes. Because if people with SSD are assaulted frequently (which they are. Please see my post on stigmatization and the media.) I think that might tie into any perceived violence as people with SSD become physically defensive.
The researchers are sold on their study: “Adherence [to treatment] is important, but the first step toward violence prevention is a high-quality risk assessment,” Fazel said. His research team has developed a free web-based risk calculator that helps clinicians estimate the risk of a patient becoming violent.
A researcher not involved in the study carefully said, “This kind of assessment, in my experience, is rarely performed in most evaluations of individuals with psychotic symptoms or SSD.” This would be the experts pushing back. The fact that such a calculator exists disgusts me, but I suppose doesn’t surprise me.
In my stigmatization and the media post I mention that attitudes to major depression have improved while attitudes to schizophrenia have worsened. “The most effective approach to reducing stigma is to “face the evidence and then avoid the negative results,” Fazel said.” Spoken like a true researcher and not a real clinician. Spoken like someone firmly outside the sphere of mental illness despite studying it. Spoken like someone who has never been close with someone with SSD. Someone whose studies are flawed anyway. Who is this someone? He’s a professor of forensic psychiatry and honorary consultant forensic psychiatrist at Oxford University:
By applying epidemiological methods, our team has examined a number of key questions in the area of forensic psychiatry and psychology. Using population-based datasets and family-based designs, this work has clarified the contribution of the main neuropsychiatric conditions to violent crime.
This seems questionably ethical when you aren’t using controls or asking the right questions. Again, how many “violent schizophrenics” were assaulted before they became violent? It is rather a germane question.
What about controls for those in your criminal registry? Why do you think a 35-year follow-up would eliminate the fact that something got this demographic into the criminal system in the first place? My guess is lack of meds and a whole lot of abuse, misunderstanding, and then strong-arming by the authorities. But I doubt these are fields in Fazel’s initial questionnaires.
“The research on schizophrenia, bipolar disorder, attention-deficit hyperactivity disorder, and epilepsy has contributed to national clinical guidelines.” I think I’ve mentioned how poor the UK’s approach to mental health is. It is completely inaccessible, and I would probably die before being treated appropriately by the NHS. Actually, it’s more likely that I actually would die just waiting for an NHS appointment. A couple of years ago a report showed that thousands actually do.
This is what happens when you reduce SSD a checkbox. However, it is not a checkbox, and Fazel is way out of line to suggest his “facts” are the way to reduce stigma. What a ridiculous notion anyway. When have “facts” ever changed a stigma? Evolving the narrative is the only way to reduce stigma. And it looks like we now have some extra work to do. And whenever the types of studies that Fazel conducts come out they are often stripped of essential meaning.
Ronald W. Pies, MD, Professor Emeritus of Psychiatry at SUNY Upstate Medical University in Syracuse, New York, who commented on the findings for Medscape Medical News notes, “The risk is not so much that these kinds of studies are conducted and then covered in the media, but that they are decontextualized and reduced to ‘bumper sticker’ headlines.” Additionally Pies says, “While the potential for violence is certainly a pertinent consideration when assessing individuals with schizophrenia spectrum disorder, it would be wrong to conclude from this study that schizophrenia spectrum disorders in themselves cause people to become violent.”
The issue of how “violent” people with SSD (or other mental illnesses) will not be solved in these pages. Stay tuned for a post dedicated to this particular topic. It’s important for everyone to know that researchers are not without their own bias. Additionally, it’s surprising how many coincidences there are in this random, chaotic world. And just because we see a result like “people with SSD are more likely to be violent” doesn’t mean that there is causation establishing settled science. You should be more worried than the average boozer in your bar than someone with SSD who is on their meds.
To conclude, stigmatization against the mentally ill has been a problem since recorded history. From the origins of stigma in Greco-Roman slavery, to the horrors of the sanatoriums, PMI have been cast out of society for the reason that they have a medical mental illness. The Church has been one of the biggest persecutors, and continues to play an active role in stigmatizing PMI to this day. Although patients’ rights have come a long way, there remain challenges, from scientists studying violence in persecuted populations, to MAGA parents stigmatizing swaths of children with a single ignorant comment.
References
[1] https://doi: 10.1111/1468-4446.12667
[2] https://doi.org/10.2307/300578
[3] https://stigmamachine.com/2020/01/20/the-ancient-penal-history-of-stigma/
[4] https://www.cugmhp.org/five-on-friday-posts/mentally-ill-in-ancient-rome/
[5] Ibid.
[6] https://en.wikipedia.org/wiki/Galen
[7] https://doi: 10.2307/1906617
[8] DOI: 10.1017/s0033291700015105
[9] https://about-history.com/the-cruel-way-people-with-mental-handicaps-were-treated-in-the-middle-ages-will-make-your-stomach-turn/
[10] Ibid.
[11] https://doi.org/10.15252/embr.201643041
[12] https://annals-general-psychiatry.biomedcentral.com/articles/10.1186/1744-859X-6-8
[13] Ibid.
[14] https://www.kqed.org/news/11209729/did-the-emptying-of-mental-hospitals-contribute-to-homelessness-here
[15] Ibid.
[16]https://www.mentalhealth.org.uk/blog/our-history-and-future-70-years-mental-health-foundation
[17] https://www.townandcountrymag.com/society/tradition/news/a9930/ted-kennedy-ptsd-patrick-kennedy/
[18] https://www.csmonitor.com/USA/Justice/2021/0518/From-LA-jail-two-inmates-pioneer-care-for-mentally-ill-peers
[19] https://www.sacbee.com/opinion/article256693562.html
[20] https://doi:10.1001/jamanetworkopen.2021.40202
[21] https://news.iu.edu/stories/2021/12/iub/releases/21-stigma-around-depression-drops-first-time.html
[22] https://www.nbcnews.com/news/us-news/parents-protesting-critical-race-theory-identify-new-target-mental-hea-rcna4991
[23] https://www.nbcnews.com/news/us-news/parents-protesting-critical-race-theory-identify-new-target-mental-hea-rcna4991
[24] https://www.cdc.gov/childrensmentalhealth/features/school-aged-mental-health-in-communities.html#:~:text=A%20CDC%20study%20examined%20mental,varied%20among%20the%20different%20sites.
[25] https://www.researchgate.net/figure/A-visual-representation-of-stigma-domains-and-their-respective-themes_fig2_317143770
I was very pleased to find this site. I wanted to thank you for your time for this particularly wonderful read!! I definitely savored every little bit of it and i also have you book-marked to see new stuff in your site.
Given the chance thast injection-site therapeutic massage can increase swrum insulin in addition to decrease blood glucose, more understaning is needed abvout the appropriate timing of pre-massage insulin injection as well ass concerning the variations within the potential risks
and benefits to people with kind 1 versus kind 2 diabetes.
Fibromyalgia pain and substance p lower and sleep
improves after therapeutic massage therapy. In case, you could have felt that thhe ache and ecstasy have taken a tokll iin your well being
and properly-being and you want the a lot-needed relaxation and refreshment, a comforting maswsage
is oone thing that you just deserve. Or
you just need a decadent hour of pure relaxatio to sooghe your
physique and restore your sense of calm. However, widespread sense can forestall potfential problems.
However, essential questions remain unanswered.
However, these statistics were not supplied. However, if therapeutic massage concomitantgly induces
a precipitous drop in blood glucose into tthe hypoglycemic fairly than the
normoglycemic range in patients using hypoglycemic medications, thgis would be an undesirable effect.
Feel free to visit my web blog https://nikkirain.com/
En visitant casino megawin, j’evalue la facon dont les jeux sont classes, surtout les slots et les jeux populaires. J’aime quand tout est logique et simple a parcourir. La fluidite sur smartphone est importante. Cela montre la qualite globale.
https://shorturl.fm/auqSy
Pour moi je reviens sur la roulette dans machine https://blooder.net/read-blog/167916 cest moyen ca vaut le
https://shorturl.fm/RQ9NB
https://shorturl.fm/2H7A0
https://shorturl.fm/tslGk
https://shorturl.fm/vNLzq
https://shorturl.fm/PR4FE
https://shorturl.fm/1zcbE
https://shorturl.fm/xrz1n
https://shorturl.fm/VALZT
Been hitting up quang88bet lately. What do you guys think? Any other recommendations? I saw good odds here: quang88bet is all I need.
Apaldo 888, never heard of her! Is it laggy or smooth? Please share your apaldo experience apaldo 888.
Bunny Casino sounds fun! Hope the payouts are real and not just carrot sticks… Get lucky bunny casino.
https://shorturl.fm/FrDSK
https://shorturl.fm/xCJnw
https://shorturl.fm/IKc7b
https://shorturl.fm/YLRrb
Anyone tried hm88game lately? I am thinking about it. Can’t really say much more because I haven’t tried it but planning to do this weekend. What are your experiences?! Click to check it out! hm88game.
Alright, I gave hubet7799 a quick glance. Site is kinda basic, but I didn’t find anything really worth noting. Just check them out! hubet7799.
Alright dudes, Jili77login’s the place to be, yeah? Super easy to get in and start playing. Good times all around! Check it: jili77login.
https://shorturl.fm/2SS9I
Just landed on 19win. Looks pretty slick! Going to poke around and see what kind of games are available. Give it a look: 19win
Looking for new online game platforms, anyone had good expereinces with”plataformadejogos“? Share the opinions!
Heard “sut88bet” is giving out some killer bonuses right now. Gonna check it out and see if it’s legit.
https://shorturl.fm/bBOCE
https://shorturl.fm/makKG
https://shorturl.fm/aB0di
https://shorturl.fm/JuqVs
https://shorturl.fm/UiYK2
https://shorturl.fm/8cJcp
https://shorturl.fm/rAE31
Anyone into the lottery? xsktangiang looks like it could be interesting. Might grab a ticket and see what happens! Check it: xsktangiang
For my fellow Filipinos, the slot vip ph login is hassle-free. Been playing here for a bit and haven’t had any issues. Sulit! slot vip ph login
Sweet, Nustar online accepts Gcash! Makes things so much easier for deposits and withdrawals. A must for Filipinos! Gcash login link right here: nustar online gcash
https://shorturl.fm/DNJbz
One88SBS, another sportsbook huh? Well, gotta check the odds and see if theres any good value. Hope so! Could use a good win. one88sbs
PokerNowClubServer? Aye, heard that’s where the lads are headin’ for a late-night tourney. Hope their connection’s good, wouldn’t want to miss a hand due to lag. Check it out here: pokernowclubserver
SuperPH777, eh? Sounds like a buzzing place online. Hope they’ve got some good bonuses for the new lads joining and plenty of action to jump into. Find the fun here: superph777
https://shorturl.fm/P5DYs
https://shorturl.fm/FJfvn
https://shorturl.fm/Abs3Y
Been seeing a lot about khelo24match360 lately. Anyone have a referral code they want to share? Or just some general advice? Sign up or check information from khelo24match360
Alright rummy fans, has anyone tried goldsrummy? Thinking about giving it a go, but want to make sure it’s not a scam first! Play rummy at goldsrummy
Just heard about my777yono! Sounds intriguing. Has anyone had any wins? I’m always trying to find a new and enjoyable pastime. Discover more at my777yono
https://shorturl.fm/bMBka
Does your website have a contact page? I’m having a
tough time locating it but, I’d like to shoot you
an e-mail. I’ve got some recommendations for your blog you
might be interested in hearing. Either way, great site and I look forward to seeing
it expand over time.
I used to be able to find good advice from your content.
This is really attention-grabbing, You are an excessively professional blogger.
I’ve joined your rss feed and sit up for looking for more of your great post.
Also, I’ve shared your web site in my social networks
Hi there, I found your web site via Google even as
searching for a related topic, your website
came up, it appears to be like good. I have bookmarked it in my google
bookmarks.
Hello there, simply changed into alert to your weblog via Google, and located that it is really informative.
I’m gonna be careful for brussels. I will be grateful when you
continue this in future. A lot of folks will probably be benefited from your writing.
Cheers!
https://shorturl.fm/kDvgJ
Hi there, You have done a fantastic job. I will definitely digg it and personally recommend to my friends.
I am sure they’ll be benefited from this web site.
https://shorturl.fm/YBFTd